Fetal Cardiac Haemodynamics: Next Step in Fetal Monitoring
Ismail Bhorat MBChB, FCOG, PhD
[email protected]
A number of high risk obstetric conditions in particular gestational diabetes, intra-uterine growth restriction (IUGR) and pre-eclampsia have a significant impact on the fetal heart, albeit from different pathophysiological pathways that include metabolic acidosis, hypoxia and increased fetal cardiac afterload respectively. We set out in this thesis to investigate fetal cardiac function in the above conditions and its links to perinatal outcomes. The parameters used to quantify fetal cardiac function were the myocardial performance index (MPI) and the E/A ratio. Normal gestational age-adjusted reference values of the MPI were initially constructed which paved the way for its use in the clinical setting1. We determined whether the MPI and E/A ratios were altered in the above mentioned high risk conditions and if so whether these altered parameters influenced perinatal outcome.
For the first time a link between fetal cardiac dysfunction, as measured by the MPI and E/A ratio, and adverse outcomes in poorly controlled gestational diabetes was established and creates for the first time a viable and reproducible fetal monitoring model to establish fetal wellbeing in poorly controlled gestational diabetes2 which hitherto standard fetal monitoring models proved ineffective in detecting fetal compromise. The reason for this is that standard monitoring models focus on placental disease and hypoxia and are not predictive of metabolic shifts and abnormal metabolic milieus in gestational diabetes where the concept of hyperlacticaemia and acidosis in the absence of hypoxia exists3. Fetal cardiac dysfunction as quantified through the MPI and E/A ratio appears to predict metabolic shifts and abnormal metabolic mileus in diabetic pregnancies2 and could serve as a guide to clinicians to establish timing of delivery and thus reduce perinatal morbidity and mortality.
We have also shown that the MPI and E/A ratios in IUGR fetuses are altered and we have established cut-off values for adverse perinatal outcome that may dictate intervention4. The unique property of the MPI is that it can easily be tracked and becomes abnormal before hypoxia or acidosis sets in and as such this parameter can be used as a monitoring tool for assessing deteriorating cardiovascular function in IUGR fetuses, thereby potentially guiding the physician to optimal timing of delivery before overt acidosis, myocardial necrosis or perinatal death sets in.
In severe early onset pre-eclampsia fetal cardiac function was significantly impaired, deteriorating with worsening placental vascular resistance and cut-off MPI values for prediction of adverse perinatal outcome and perinatal death have been established (paper submitted for publication). To our knowledge this is the first work in pre-eclampsia demonstrating the value of categorizing resistance to blood flow with the degree of cardiac dysfunction.
This thesis has provided evidence that fetal cardiac function, as quantified by the MPI and E/A ratio, can potentially be integrated into routine antenatal surveillance techniques in the above high risk obstetric conditions enabling clinicians in decision-making regarding timeous delivery and thereby reducing perinatal morbidity and mortality.
References:
-
Bhorat I, Bagratee R, Reddy T. Gestational age-adjusted trends and reference intervals of the myocardial performance index and its components with its interpretation in the context of established cardiac physiological principles. Prenatal Diagnosis:2014;34 (11): 1031-1036
- Bhorat I, Bagratee J, Pillay M et al. Use of the myocardial performance index as a prognostic indicator of adverse fetal outcome in poorly controlled gestational diabetic pregnancies. Prenatal Diagnosis 2014; 34(13): 1301-1306
- Bradley RJ, Brunedell JM, Nicolaides KH. Fetal acidosis and hyperlacticaemia diagnosed by cordocentesis in pregnancies complicated by maternal diabetes mellitus. Diabet Med 1991;8:464-468.
- Bhorat I, Bagratee J, Pillay M, Reddy T. Determination of the myocardial performance index in deteriorating grades of growth restriction and its link to adverse outcomes. Prenatal Diagnosis: 2015:35(3); 266-273
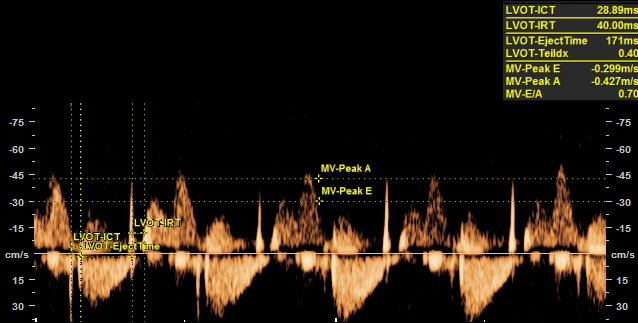
Normal myocardial performance index and E wave/A wave peak velocity ratio Doppler tracing at the mitral valve.
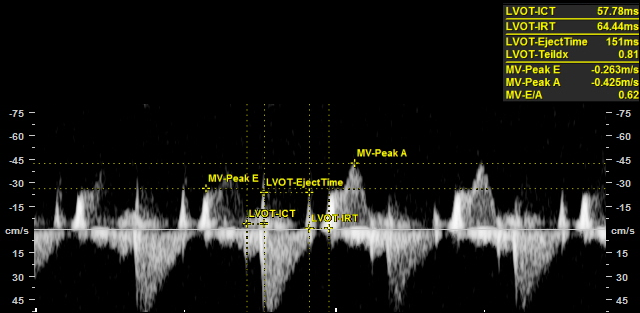
Abnormal myocardial performance index and E wave/A wave peak velocity ratio Doppler tracing at the mitral valve